The Future of Pediatric ICU
Cornell University * NYP Pediatric ICU
Instructor
Dr. Rana Zadeh
Department of Design and Environmental Analysis, Cornell University
Partnering with
New York Presbyterian Hospital's Pediatric Intensive Care Unit
Student Innovators
Mio Jia, Nicole Shana Levine, Hanchun Shao, Cameron McKee (Team 2)
(6 teams total) this page only present Team 2's final innovations
Sponsors
New York Presbyterian Hospital's Pediatric Intensive Care Unit, Cornell Institute for Healthy Futures and the Department of Design & Environmental
Hospital Visit


Goal 01 Improve Patient Safety
Objective: Improve safety through standardizing information transfer and communication protocols with focused attention on patient handover processes
Strategy 1.1
Ensure that there is a multiplicity of simultaneous strategies for information transfer so that all clinical patient and staff needs are addressed in handovers (short term)
Research demonstrates that bundled interventions regarding communication protocols in patient handovers result in improved quality and perception of quality (Clark et al., 2009). A system integrating multiple approaches protects patients from errors resulting from lack of communication and misunderstanding. Standardizing such a system helps ensure that steps will consistently and diligently be followed (Moon et al., 2016).
Strategy 1.2
Use different mediums for communication to reduce gaps in logistics and clinical needs (short term)
Effective bundles of different mediums include verbal cues, mnemonic devices, face-to-face meetings, electronic information, and streamlined form documentation. “Medical errors decreased from 33.8 per 100 admissions (95% CI, 27.3-40.3) to 18.3 per 100 admissions (95% CI, 14.7-21.9; P < .001)” (Starmer et al. 2013).
Electronic access to information is especially critical for night and weekend staff. (Govier & Medcalf, 2012) Electronic information integrates with EHRs, providing staff attending to a patient with direct access to the patient’s medical history. Time spent in cumbersome turnover processes is reduced, and there is a backed up, secure version of the necessary information (Maher et al., 2013).
Strategy 1.3
Integrate information on a clear timeline (short term)
The more standardized and clear a process is, the less room for error there is. In a 2016 study, having a clear protocol integrated into the handover process increased the perceived effectiveness of the handover (Moon et al., 2016). This can include developing checkpoints such as pre-patient, pre-transfer, and post-transfer information debriefings (Moxey et al., 2016). Such checkpoints make sure that all staff involved in a handover are ready and equipped for next steps without ambiguity. Misunderstanding complex goals of patient care can jeopardize safety (Reader et al., 2016).
Room for potential error can be minimized through standardization of communication and combination of methodologies into a comprehensive checklist protocol that is intuitive to the care process. A study on decreasing catheter-related bloodstream infections in 2006 supported the idea that checklists ensure adherence to infection control procedures. It is imperative that a formalized structure exists to enforce such procedures so staff members can hold each other accountable at all levels (Provonst et al., 2006).
Strategy 1.4
Ensure that communication protocols meet personnel needs (short term)
1.4.1 Implement interdisciplinary communication standards
All staff involved in patient care should be aware of the patients’ clinical needs and medical histories. The team treating the patient is collaborative between nurses, doctors, and other medical staff, and information must be suitable for each of their tasks. Doctors in positions of hierarchy report better levels of communication than do other staff members. Creating a structured protocol for information delivery between all types of medical staff will clarify expectations and patient care goals (Reader et al., 2007)
1.4.2 Use information transfer protocols such as night huddle to reduce errors on nights and weekends (Short term)
A disproportionate amount of safety risks occur at night and on weekends. Research demonstrates that the most frequent type of accident is falling which mainly occurred during the night (Da Rin Della Mora et al., 2012). Time of admission is also correlated with mortality rates (McCrory et al., 2017; Rehder et al., 2015).
Night shifts are correlated with lack of supervision from an attending physician, which intensifies risk. Therefore, protocols for night staff should protect patients from gaps in care that could result from short staffing and lack of face-to-face meetings between staff. One study proved that use of a night huddle protocol decreased high-risk transfers in the ICU (Newman et al., 2016). The method used in this study was as follows:
“The huddle starts with a rounding process between the overnight residents and bedside nurses at ~9:00 pm, followed by a conference call among the residents, charge nurse, and at-home cardiologist to review all patients on the team and discuss any needed immediate patient care needs as well as contingency plans.”
Furthermore, the study demonstrated that this protocol generally opened lines of communication between staff.
Design innovations
Design innovation: Increase flexible and efficient storage; Reduce acoustic stimuli and distractions

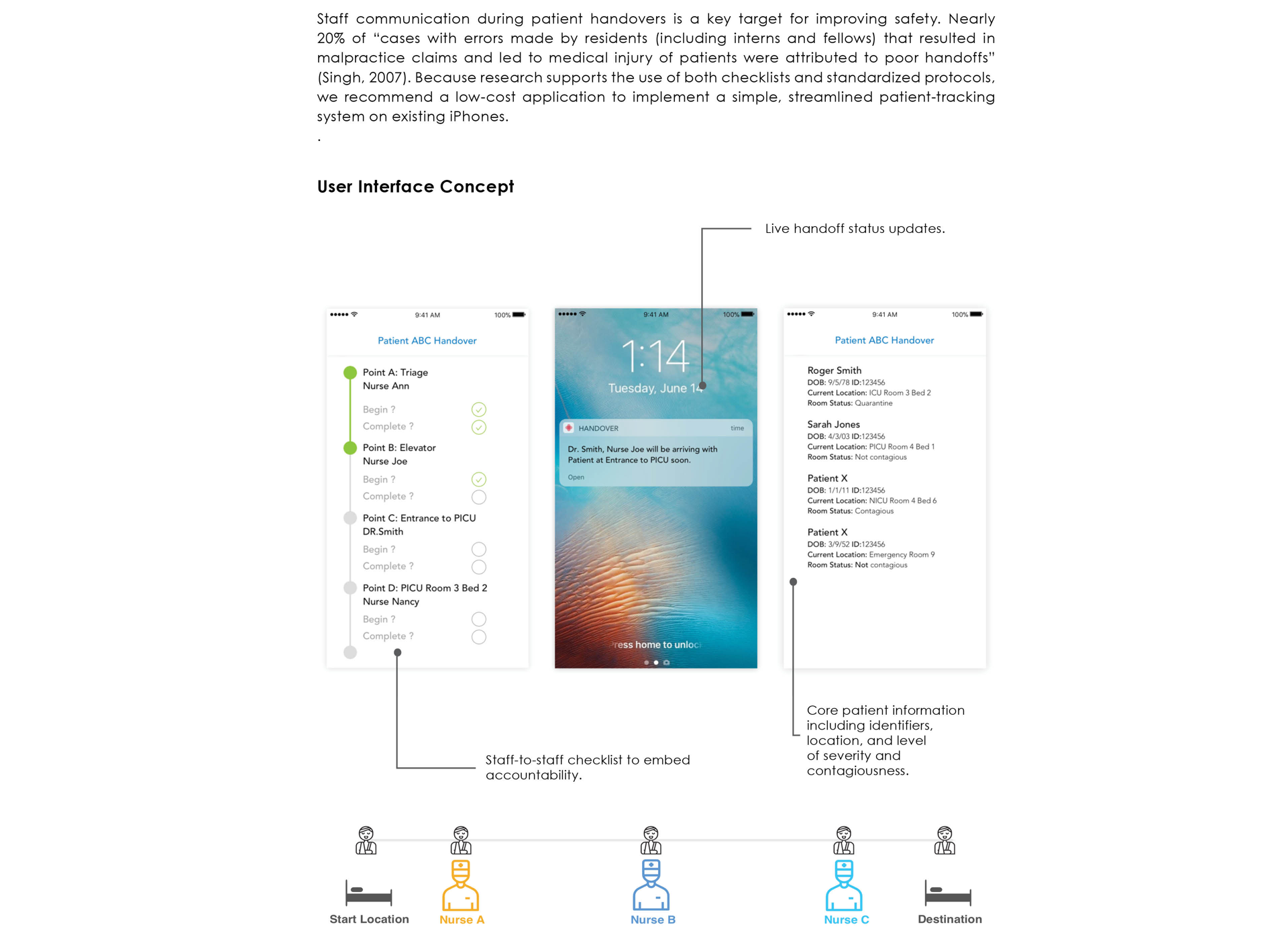
Design innovation: standardize handover communication
Design innovation:Increase patient confidentiality and control acoustic disturbances; Provide a personalized and home-like environment

Design innovation:multi-patient-room noise reduction

Goal 02 Staff Satisfaction through Environmental Interventions
We will help staff experience more fulfilling work, and be less prone to burnout by enhancing resource management and reducing, creating a more organized and friendly work environment. Staff satisfaction can improve performance and therefore increase hospital success and productivity.
Strategy 2.1
Use sound absorbing materials to reduce ambient noise and improve acoustics to boost staff’s environmental satisfaction
2.1.1 Using transparent walls and automatic sliding doors significantly decreases noise level (long term)
With noise coming from a host of sources in an ICU (nursing stations, alarms, visitors, bedside conversations, etc.), individuals must compete to be heard. Implementing easily movable permanent partitions significantly reduces noise (Kol, 2015).
2.1.2 Carpet tile is an ideal floor covering for sound absorption (long term)
Carpet tile has shown to be the best floor material to reduce noise by up to 3.14 dBA compared to traditional hospital flooring and has been shown to increase satisfaction in hospital staff and patients (Harris, 2015; Konkani et al., 2014). Additionally, carpet has been shown not to transmit infections to staff or patents (Harris, 2010). Research shows that excessive noise is a detrimental factor that can increase fatigue, increase anxiety and stress, decrease productivity, and decrease workplace satisfaction in hospital staff (Thiel et al., 2014). Reducing noise via sound-hampering materials will therefore make work more enjoyable for employees, reducing perceived workload.
2.1.3 Sound absorbing ceiling tiles improve patient room acoustics. (short term)
Sound-absorbing tiles cut reverberation time in half compared to reflecting tiles. Additionally, in comparison to sound-reflecting ceiling tiles, sound-absorbing tiles increase staff satisfaction by decreasing perception of work demands, pressure, and stress (Blomkvist et al., 2005). This improved acoustic work environment improves psychological well-being of nurses and doctors, leading them to complete better work (Konkani & Oakley, 2012).